For patients with atrial fibrillation who are at risk of stroke but cannot safely take long-term blood thinners, left atrial appendage occlusion offers a durable alternative — sealing off the small pouch where most AF-related clots form, and reducing stroke risk without lifelong anticoagulation.
Atrial fibrillation (AF) is the most common heart rhythm disorder, and one of its most serious consequences is stroke. In AF, the upper chambers of the heart quiver rather than contract effectively, allowing blood to pool and clot — most often in a small, finger-like pouch called the left atrial appendage (LAA). If a clot forms there and travels to the brain, it causes a stroke.
The Problem with Anticoagulation
The standard treatment to prevent AF-related stroke is oral anticoagulation — blood-thinning medication such as warfarin or a direct oral anticoagulant (DOAC). These drugs are highly effective. But some patients cannot take them safely: those with a history of major bleeding, those at high risk of falls, those with certain gastrointestinal or intracranial bleeding risks, or those who simply cannot tolerate the medication. For these patients, the very treatment meant to protect them creates a different danger.
How LAA Occlusion Works
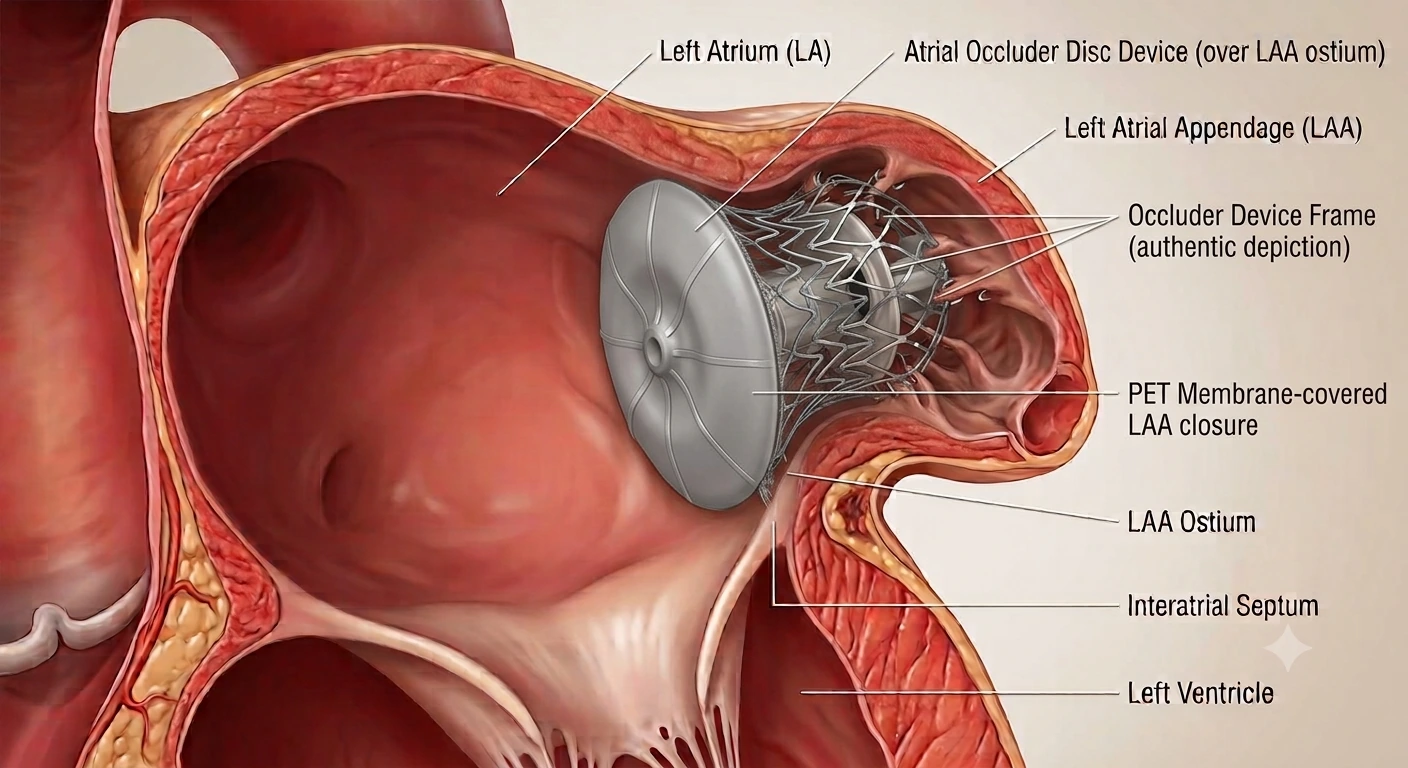
Because the vast majority of AF-related clots form specifically in the left atrial appendage, sealing off this pouch can dramatically reduce stroke risk. LAA occlusion is a catheter-based procedure: a device (such as the WATCHMAN FLX or Amulet) is delivered through a vein in the groin, guided across the atrial septum into the left atrium, and deployed at the mouth of the appendage — effectively closing it off from the circulation. Over time, tissue grows over the device, permanently sealing the pouch.
The procedure is guided by echocardiography and X-ray, performed under sedation or general anaesthesia, and typically takes around an hour. Most patients stay one night in hospital.
"For the AF patient who bleeds on anticoagulation, LAA occlusion changes the equation entirely — protecting against stroke without the constant risk of the medication meant to prevent it."
— Dr. Zaidoun Hajali, MD FSCAI FRCPThe Evidence
The PROTECT AF and PREVAIL trials established that WATCHMAN LAA occlusion is non-inferior to warfarin for stroke prevention in suitable AF patients, with the added benefit of reduced long-term bleeding risk. Subsequent registries and the newer-generation devices have reinforced the safety and effectiveness of the approach. It is now an established option recommended in international guidelines for AF patients with contraindications to long-term anticoagulation.
Who Is a Candidate?
LAA occlusion is primarily considered for patients with non-valvular atrial fibrillation who have an elevated stroke risk but a compelling reason to avoid long-term anticoagulation — most commonly a history of serious bleeding or a high bleeding risk. The decision is individualised and made after careful assessment of stroke risk, bleeding risk, and the patient's own preferences.
- Most atrial fibrillation-related clots form in the left atrial appendage (LAA) — sealing it reduces stroke risk.
- LAA occlusion is a catheter-based alternative for AF patients who cannot safely take long-term blood thinners.
- A device (WATCHMAN FLX, Amulet) is delivered through a vein and deployed at the mouth of the appendage.
- The PROTECT AF and PREVAIL trials showed non-inferiority to warfarin with reduced long-term bleeding.
- Ideal candidates have non-valvular AF, elevated stroke risk, and a strong reason to avoid anticoagulation.
