After many years in the cath lab, I have learned exactly when the kissing balloon is worth using in left main PCI — and when reaching for it reflexively turns a successful case into a problem. The answer is not intuitive, and it is not the same for every strategy. The CFD data makes it clear.
The kissing balloon inflation (FKB) in left main bifurcation PCI is one of the most debated technical decisions in interventional cardiology. Should you always do it? Never? Only sometimes? The answer depends entirely on whether you are working with a 1-stent or a 2-stent strategy — and the hemodynamic rationale for each decision is now backed by both computational fluid dynamics (CFD) modelling and randomised trial data.
What Is the Kissing Balloon and Why Does It Matter?
In bifurcation PCI, the kissing balloon inflation (FKB) refers to the simultaneous inflation of two balloons — one in the main vessel and one in the side branch — after stent deployment. The technique is designed to optimise the stent geometry at the bifurcation point, re-open the side branch ostium, and restore the natural flow dynamics at the carina.
In left main PCI specifically, the stakes are exceptionally high. The left main coronary artery supplies blood to the majority of the left ventricular myocardium. A poor result at the distal left main bifurcation — inadequate stent expansion, carina distortion, or flow limitation in the circumflex — can have serious clinical consequences. This is why the technical decisions here are not trivial, and why the CFD data matters.
1-Stent Strategy — Put the Kissing Balloon Down
The scenario: an operator finishes a clean left main stent. The angiographic result looks good. Then — almost reflexively — a second wire is advanced into the circumflex and a kissing balloon is performed, "just to make sure."
That decision just turned a successful case into a potential problem.
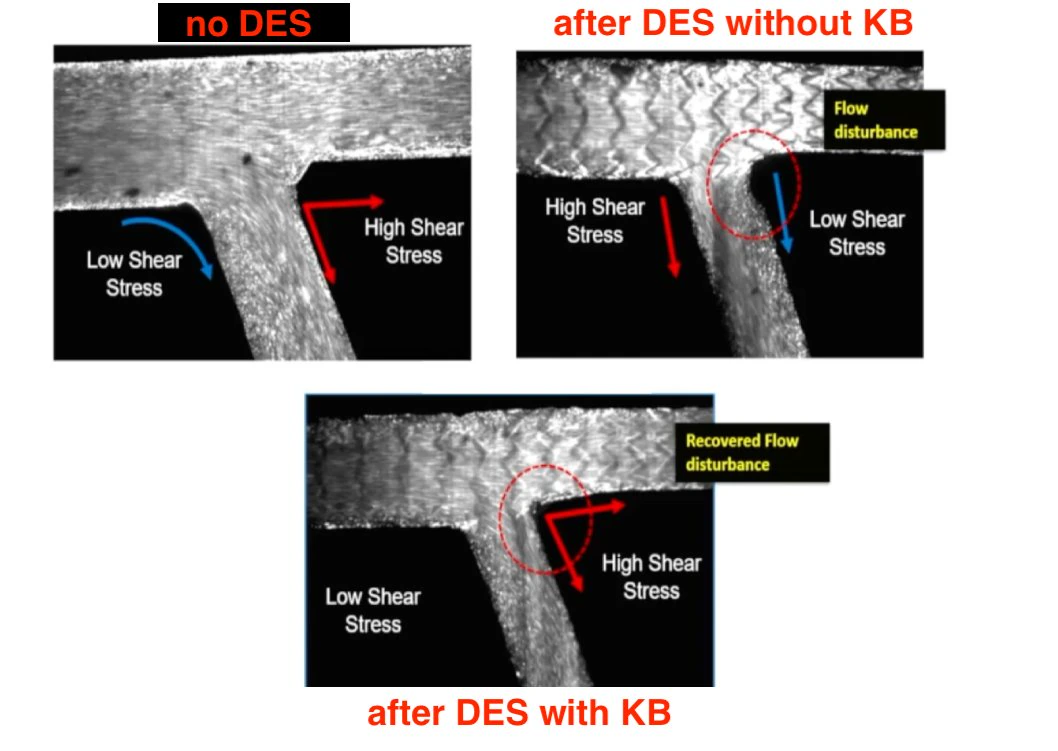
Routine final kissing balloon in a 1-stent provisional strategy carries no documented benefit — and carries real risk. The CFD data shows exactly what happens: when the bifurcation geometry is disturbed by balloon inflation in a side branch that was previously stable, you create carina distortion and flow disturbance in a zone that did not need to be touched. The shear stress distribution — previously acceptable — becomes abnormal. Low shear stress zones appear at the circumflex ostium precisely where you have just inflated. This creates the substrate for neointimal hyperplasia and restenosis.
There is also a practical cascade risk: disturbing the side branch ostium frequently prompts the operator to place a second stent that was never part of the plan. A provisional 1-stent case becomes a 2-stent case not because the anatomy required it, but because the kissing balloon created a problem that then seemed to need fixing.
"My rule: if the side branch has acceptable flow and IVUS confirms adequate main branch expansion — close the case. The only reason to touch the side branch is stenosis or flow limitation that demands it."
— Dr. Zaidoun Hajali, MD FSCAI FRCP2-Stent Strategy — Now You Must Kiss. No Negotiation.
The same shear stress physiology that argues against FKB in a 1-stent case argues strongly for it in a 2-stent case. After two stents have been deployed at the left main bifurcation, a neo-carina is created at the junction. This neo-carina generates a flow disturbance zone — visible in the CFD modelling — that does not resolve on its own. Without kissing balloon, that zone of disturbed flow and low shear stress becomes a nidus for restenosis.
FKB in a 2-stent case restores the bifurcation geometry. The hemodynamic recovery is visible in the CFD data: flow disturbance at the carina is resolved, shear stress distribution normalises, and the side branch is properly scaffolded. TVR and TLR event rates track in the same direction as the hemodynamics.
There are three non-negotiables when performing FKB in a 2-stent left main case:
First: use short balloons to minimise overlap in the proximal main vessel. Excessive overlap creates its own problems with stent geometry proximal to the bifurcation.
Second: FKB is the closing step of every 2-stent case — not a decision made at the end based on how the angiogram looks. It should be planned from the start.
Third: sequence matters enormously. The PKP sequence — POT → kissing balloon → final POT — outperforms the PSP sequence (POT → side branch only → final POT).
The CRABBIS Trial — Why PKP Wins
The CRABBIS trial is the first randomised study to directly compare these two ballooning sequences in left main and large coronary bifurcations. The primary endpoint — minimum stent expansion at the distal main vessel on OCT — was significantly better with the PKP sequence. Additional findings showed higher rates of stent malapposition in the bifurcation core and distal main vessel with PSP, and improved side branch scaffolding with PKP.
The mechanism is straightforward: isolated side branch dilation (PSP) causes carina shift towards the main vessel, deforming the stented areas near the carina and leading to incomplete expansion and apposition at the distal main vessel. Simultaneous kissing balloon inflation (PKP) maintains the central position of the carina, preventing this deformation and achieving more uniform stent expansion.
Why IVUS Is Not Optional in Left Main PCI
The entire decision framework described above — whether to touch the side branch, whether to close the case, whether the main vessel is adequately expanded — depends on having objective data, not just an angiographic impression. And that objective data comes from IVUS.
In a 1-stent left main case, IVUS is how you confirm that the main branch is adequately expanded before deciding to close. Without it, you are guessing — and guessing in one of the highest-stakes territories in interventional cardiology is not acceptable. IVUS tells you whether your one stent actually did its job. If expansion is adequate and the side branch has acceptable flow, close the case. If not, IVUS tells you what still needs to be done.
In a 2-stent case, IVUS (or OCT) is essential to confirm the result of the kissing balloon, identify any residual underexpansion, and guide the final POT. The CRABBIS trial used OCT at every step precisely because the geometry changes at each stage of the PKP sequence are real and measurable — and they matter for outcomes.
- 1-stent strategy: resist the urge to kiss if there is no flow limitation and IVUS confirms adequate main branch expansion. Close the case.
- 2-stent strategy: you must perform kissing balloon to finish the job. Use the PKP sequence. This is not optional.
- The decision is not made on the table — it is made before the first wire goes in, based on the anatomy and the planned strategy.
- IVUS is not optional in left main PCI. It is how you know whether your stent did its job.
- Use short balloons for kissing — minimise proximal main vessel overlap.
- PKP (POT → kissing → final POT) outperforms PSP. The CRABBIS trial confirms this with OCT data. Bianchini F et al. JACC Cardiovasc Interv. 2025.
