A chronic total occlusion is a coronary artery that has been completely blocked for at least three months. Reopening one is the most technically demanding procedure in interventional cardiology — requiring specialised techniques, dedicated equipment, and considerable operator experience. For the right patient, the benefit can be transformative.
A chronic total occlusion (CTO) is a coronary artery that is 100% blocked and has been for an extended period — by definition at least three months. Unlike an acute blockage, a CTO develops gradually, and the heart often adapts by growing small collateral vessels that provide some blood supply to the affected territory. But these collaterals are rarely sufficient, and patients frequently experience angina, breathlessness, and reduced exercise capacity.
Why Open a CTO?
The goal of CTO PCI is to relieve symptoms and improve quality of life. Many patients with a CTO live with chronic angina or exertional breathlessness that limits their daily activities, often without realising how much they have adapted their lives around the limitation. Successful CTO opening can dramatically improve symptoms, exercise capacity, and — in selected cases — the function of the heart muscle supplied by the blocked artery.
The decision to attempt a CTO is individualised. It depends on the severity of symptoms, evidence that the affected heart muscle is still viable (and would benefit from restored blood flow), the complexity of the occlusion, and the patient's overall clinical picture. It is not undertaken lightly, and it is best performed by operators with specific CTO expertise.
The Techniques
CTO PCI has evolved into a sophisticated discipline with a structured approach — the hybrid algorithm — that guides operators through several strategies. The antegrade approach works forward through the blockage from the proximal end, using specialised guidewires to cross the occlusion. The retrograde approach works backwards, accessing the occlusion from the far side via collateral channels — an elegant but demanding technique used when the antegrade route fails. Dissection and re-entry techniques create a controlled plane through the vessel wall to bypass the hardest segments.
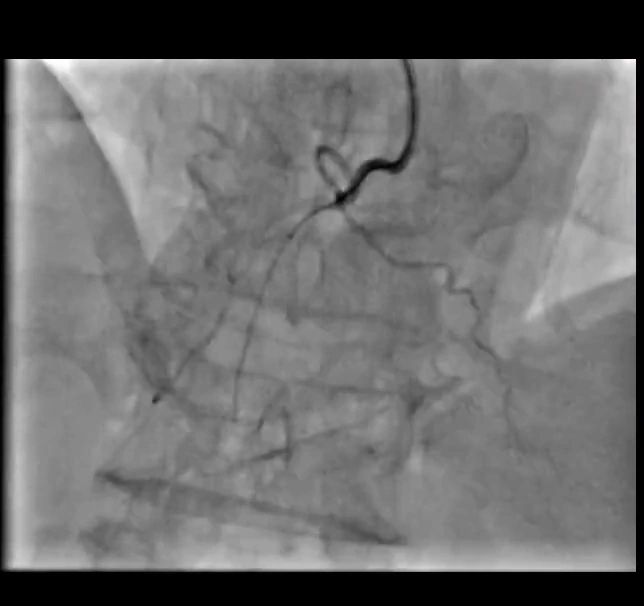
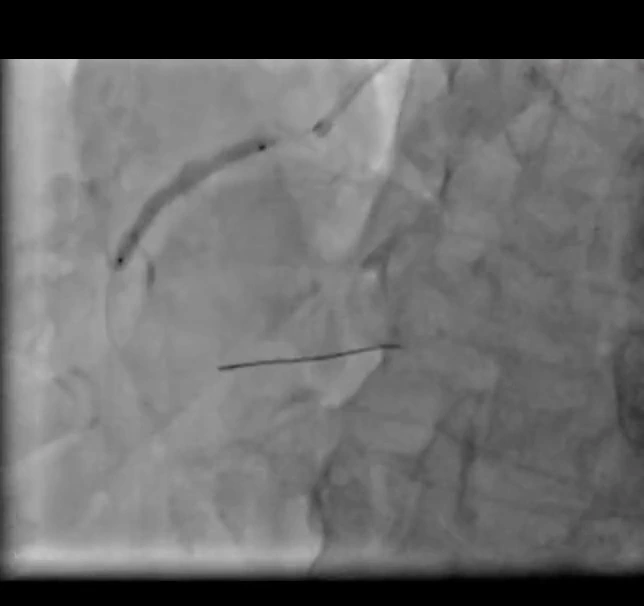
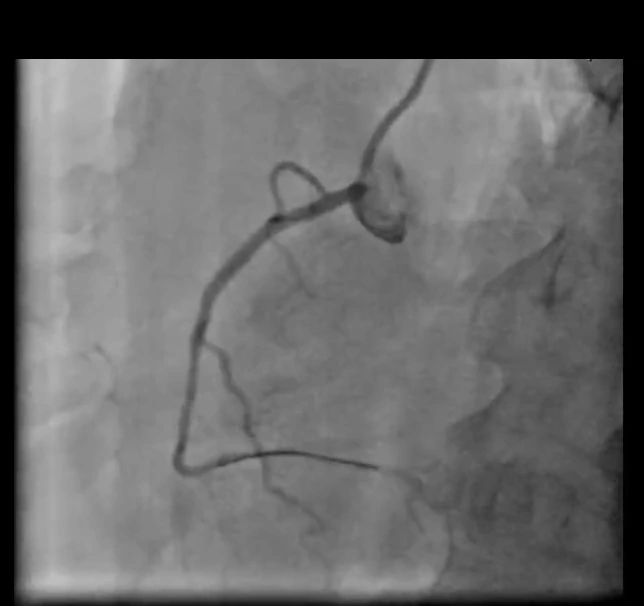
Antegrade CTO recanalisation of the right coronary artery
Angiographic sequence · LAO 30°

"CTO PCI is a discipline of patience and strategy. Success comes not from force, but from having a clear algorithm, the right equipment, and the experience to move seamlessly between techniques."
— Dr. Zaidoun Hajali, MD FSCAI FRCPSpecialised Equipment
CTO procedures rely on dedicated equipment: a wide array of specialised guidewires with different tip stiffness and coatings, microcatheters that support and direct the wires, and re-entry devices. Intravascular imaging and, increasingly, CT angiography help plan the approach in advance. The procedure can take considerably longer than a standard PCI and may use more contrast and radiation, which is why patient selection and operator experience are so important.
What Results to Expect
In experienced hands, contemporary CTO PCI achieves success rates of 85–90% or higher. When successful, patients often report significant improvement in angina and exercise tolerance. As with any complex procedure, there are risks, and these are discussed in detail beforehand. The key is realistic expectation-setting: CTO PCI is primarily a quality-of-life procedure, and the decision should always weigh the expected symptomatic benefit against the complexity and risk in each individual case.
- A chronic total occlusion (CTO) is a coronary artery 100% blocked for at least three months.
- CTO PCI is primarily performed to relieve angina and breathlessness and improve quality of life.
- The hybrid algorithm guides operators between antegrade, retrograde, and dissection/re-entry techniques.
- CTO procedures require specialised guidewires, microcatheters, and considerable operator experience.
- In experienced hands, success rates reach 85–90%+; patient selection and realistic expectations are essential.
